
Intramuscular Injection Buttock Hip Simulator Manikin Model
Buyamag INC
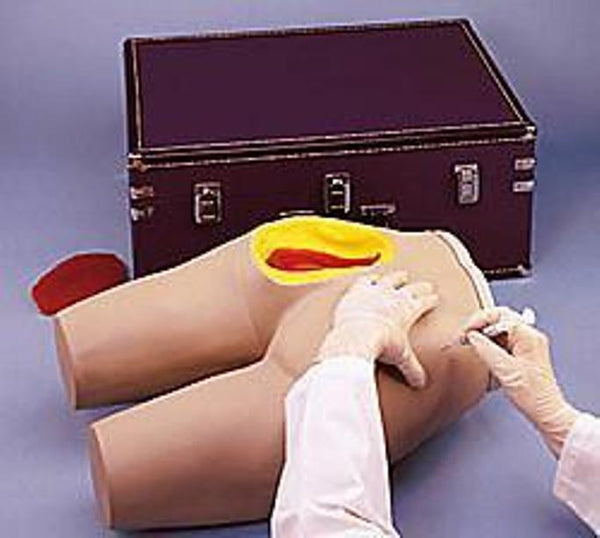
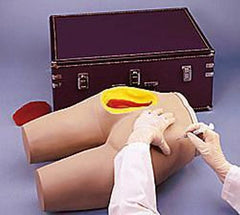
Intramuscular Injection buttock simulator model is designed to provide students with the visual and tactile experience needed to learn intramuscular injection techniques. This simulator has landmarks that can be palpated so that the various injection techniques can be practice.
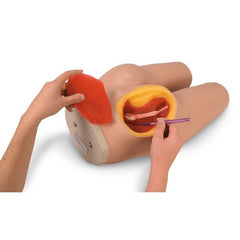
Unique design and construction give students the opportunity to visualize underlying structures and quickly learn proper injection procedures
Intramuscular Injection Simulator is extremely realistic. Skin and muscle textures and bone shape and position closely resemble a live patient.
As a result, perforation of the tissue with a needle duplicates the sensation of administering an actual injection.
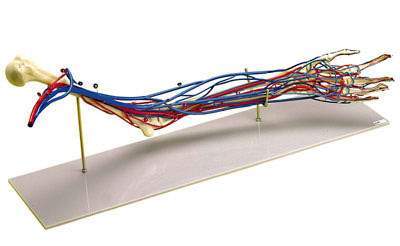
A simulated bony structure is embedded in the torso and represents the superior end of the femur or greater trochanter; the posterior superior and anterior superior iliac spines; and the sacrum. Bones are positioned in a way that students are able to visualize and palpate these anatomical landmarks in order to identify the gluteal injection sites.
A section of the upper, outer quadrant of the left gluteal area is cut away to allow students to visualize the underlying structures. The gluteus medius and gluteus maximus muscles, sciatic nerve, and vascular structures are clearly shown.
Some students, and even instructors, have found the realism of this simulator to be rather startling. It was intended to be just that. It will provide the kind of learning experience that helps students make the transition from the idealized classroom setting to the realities of ward duty.
Procedures That Can Be Performed On This Simulator
The Intramuscular Injection Simulator is a functional teaching aid that enables personnel to develop manipulative skills and improve techniques. It makes the learning experience one that is easily applied in actual patient care, with little loss of time and a minimum of patient discomfort.
The specific techniques in intramuscular injections that can be taught with this simulator are:
A. Gluteus Medius Injections
This is probably the most commonly considered site for giving posterior injections; the sciatic nerve transverses this area. If a student perforates the nerve or the vascular structures, it can cause irreparable harm to the patient. One acceptable technique for giving an injection in this site is to have the patient in a prone position, toes flexed inward. This relaxes the posterior muscles. The simulator duplicates this position. The student then identifies the greater trochanter and draws an imaginary line from it to the crest of the posterior iliac crest. An injection may be given anywhere above and outside of this imaginary plane. The needle should penetrate on a direct back-to-front route.
Another technique is to place the palm of the hand over the trochanter and extend the spread fingers towards the posterior iliac spine. An injection may be safely administered by entrance between the thumb and index finger.
B. Ventrogluteal Injections
This site is becoming more frequently used for injections because it is removed from major blood vessels and nerves, and it also presents good muscle density. Because of the previously listed features and because the landmarks are so easily identified, this site can often be used in giving pediatric injections. The patient can be injected in this area while in a prone position, on their side, or standing, but the best technique dictates that they should be in a supine position.
The student defines the site by locating the greater trochanter and placing their palm on it. Then the index finger should reach towards the anterior iliac crest. Now move the middle finger away from the index finger. The triangle between the two is the safe site to inject. The needle should be inserted towards the iliac crest at a slight upward angle.
C. Vastus Lateralis Injections
Again because of the lack of major vessels and nerves, this site is often used in pediatric patients. With the patient in the supine position, the student identifies the site by positioning one hand above the knee and one hand below the greater trochanter. The area between the hands is the safe zone.